Arterial Supply of the Foregut
Venous Drainage
- Stomach
- Duodenum
- Liver and Gallbladder
- Pancreas and Spleen
- Vascular Supply of the Foregut
- Study Questions
The duodenum curves around the pancreatic head. It is divided into the following four parts (Figure A and B):
- Part one (superior). The stomach is an intraperitoneal organ as is the first part of the duodenum. The first part of the duodenum contains the duodenal cap, a dilation of the proximal duodenum that is easily identifiable on radiographs. In contrast, the second part of the duodenum courses deep to the parietal peritoneum and thus is retroperitoneal, as are the third and fourth parts of the duodenum. However, the distal portion of the fourth part is transitional, from retroperitoneal to intraperitoneal in the region of the duodenojejunal junction.
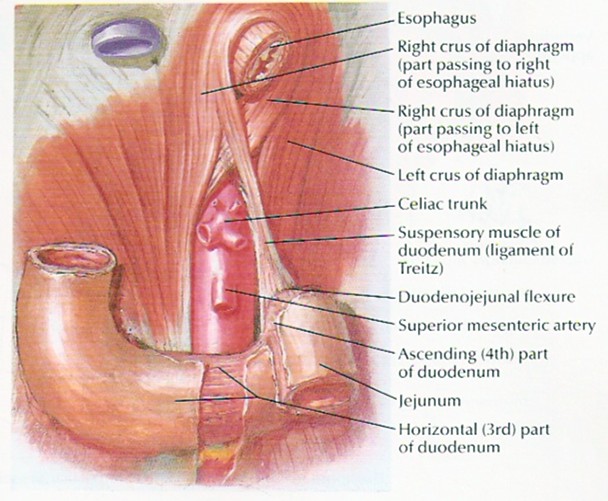
The upper gastrointestinal (GI) tract begins at the mouth and extends to the ligament of Treitz (actually not a ligament at all, but the suspensory muscle of the duodenum, which participates in GI motility). The lower GI tract includes everything distal to this point.
Of note, an upper GI bleed is a bleed proximal to the ligament of Treitz. It will usually present with hematemesis or melena (although it may present as hematochezia if very brisk). A lower GI bleed is distal to the ligament of Treitz and will usually present as hematochezia. Overall, two thirds of all GI bleeds are from an upper GI source.
- Part two (descending). Courses deep to the transverse colon and anterior to the right kidney. The common bile duct enters its posterior wall. Within the duodenal wall, the common bile duct receives the main pancreatic duct (of Wirsung). Immediately after the junction, there is an enlargement called the major duodenal papilla (ampulla of Vater). The papilla is surrounded by smooth muscle called the sphincter of Oddi. An accessory pancreatic duct (of Santorini) may enter the duodenum proximal to the main pancreatic duct.
- Part three (horizontal). Turns left and courses horizontally across the inferior vena cava, the aorta, and the vertebral column. In addition, the superior mesenteric artery and vein course anteriorly to the third part of the duodenum.
- Part four (ascending). Ascends anterior to the aorta at the L2 vertebral level.

The duodenum receives its blood supply from branches of both the celiac trunk (superior pancreaticoduodenal arteries) and the superior mesenteric trunk (inferior pancreaticoduodenal arteries).
The liver is situated under the right diaphragm in the lower part of the right rib cage.

The left lobe of the liver is in the epigastrium.
The liver is covered with visceral peritoneum over most of its surface and is suspended by several mesenteric structures called ligaments.
The falciform ligament (with the ligamentum teres at its free margin) is the embryonic remnant of the ductus venosus (umbilical vein) of the umbilical cord. It is a peritoneal structure that courses between the anatomical left and right lobes of the liver and the anterior abdominal wall.
The larger right lobe has two additional smaller lobes at its posterior-inferior surface, the caudate and quadrate lobes.
In contrast, surgical anatomy divides the liver based on its blood supply. Thus, the right and left surgical lobes are defined by the point of bifurcation of the hepatic artery and portal vein (porta hepatis); the falciform ligament therefore divides the left surgical lobe into medial and lateral segments. Surgical anatomy defines a total of eight segments.
As the falciform ligament passes onto the superior surface of the liver, the two layers of peritoneum diverge to the right and to the left, creating the anterior layers of the coronary ligaments. These pass to the right and to the left to the extremes of the superior liver surface, turn back on themselves (creating the triangular ligaments), and turn posteriorly to form the posterior layers of the coronary ligaments. In this manner, an area devoid of visceral peritoneum is created, the bare area of the liver. The posterior layers of the coronary ligaments converge to form the lesser omentum, which passes from the visceral surface of the liver to the lesser curvature of the stomach (hepatogastric ligament) and the first part of the duodenum (hepatoduodenal ligament).
The liver is covered with visceral peritoneum over most of its surface and is suspended by several mesenteric structures called ligaments.
The falciform ligament (with the round ligament of the liver, the adult remnant of the umbilical vein, in its free margin) is reflected onto the anterior abdominal wall and divides the liver into apparent right and left anatomical lobes.
As the falciform ligament passes onto the superior surface of the liver, the two layers of peritoneum diverge to the right and to the left, creating the anterior layers of the coronary ligaments.
These pass to the right and to the left to the extremes of the superior liver surface, turn back on themselves (creating the triangular ligaments), and turn posteriorly to form the posterior layers of the coronary ligaments.
In this manner, an area devoid of visceral peritoneum is created, the bare area of the liver. The posterior layers of the coronary ligaments converge to form the lesser omentum, which passes from the visceral surface of the liver to the lesser curvature of the stomach (hepatogastric ligament) and the first part of the duodenum (hepatoduodenal ligament).
The liver is divided anatomically into four lobes by external landmarks and is delineated on the visceral surface by fissures and fossae resembling an "H".
See: 3D Interactive Liver Anatomy
The right side of the "H" is formed by fossae for the gallbladder and the IVC, and the right lobe lies to the right of these structures. The left side of the H is formed by the fissure for the round ligament and the ligamentum venosum (adult remnant of the ductus venosus); the left lobe is to the left of this fissure. The crossbar of the H is the porta hepatis through which the hepatic artery, portal vein, and nerves enter the liver and the bile ducts and lymphatics exit. The crossbar subdivides the central portion into quadrate and caudate lobes. Functionally, the right portal lobe lies to the right of the fossae of the gallbladder, IVC, and a portion of the caudate lobe. The left portal lobe is the left anatomical lobe, quadrate lobe, and the remainder of the caudate lobe. The portal lobes are supplied by lobar branches of the hepatic artery, portal vein, and bile ducts. Although lacking external landmarks, the portal lobes are further divided functionally into hepatic segments.
The liver is divided anatomically into four lobes by external landmarks and is delineated on the visceral surface by fissures and fossae, which form an “H.” (See Figure Below).

The visceral surface of the liver. (Reproduced, with permission, from Lindner HH. Clinical Anatomy. East Norwalk, CT: Appleton & Lange, 1989:399.)
The right side of the H is formed by fossae for the gallbladder and the IVC, and the right lobe lies to the right of these structures. The left side of the H is formed by the fissure for the round ligament and the ligamentum venosum (adult remnant of the ductus venosus); the left lobe is to the left of this fissure. The crossbar of the H is the porta hepatis through which the hepatic artery, portal vein, and nerves enter the liver and the bile ducts and lymphatics exit. The crossbar subdivides the central portion into quadrate and caudate lobes. Functionally, the right portal lobe lies to the right of the fossae of the gallbladder, IVC, and a portion of the caudate lobe. The left portal lobe is the left anatomical lobe, quadrate lobe, and the remainder of the caudate lobe. The portal lobes are supplied by lobar branches of the hepatic artery, portal vein, and bile ducts. Although lacking external landmarks, the portal lobes are further divided functionally into hepatic segments.
The four lobes of the liver are as follows:
- Right lobe. Positioned to the right of the inferior vena cava and gallbladder.
- Left lobe. Positioned to the left ligamentum teres.
- Quadrate lobe. Positioned posterior to the portal triad.
- Caudate lobe. Positioned anterior to the portal triad.

A. Visceral (inferior) view of the liver. B. Portal triad. C. Anterior view of the foregut with the body and pylorus of the stomach removed; the lesser omentum is also removed.
Functionally, the quadrate and caudate lobes are part of the left lobe because they are supplied by the left hepatic artery, drained by the left branch of the portal vein, and deliver bile via the left bile duct.
Liver Size
Normal size — The liver is wedge-shaped. The liver typically extends from the fifth intercostal space to the right costal margin in the midclavicular line. The size of the liver increases with age, from an average span of 5 cm at the age of five years, to 15 cm in adulthood [1]. The size of the normal liver also varies with sex and body size [2-4]. The normal liver weighs 1.4 to 1.5 kg in men and 1.2 to 1.4 kg in women [1]. Relative to body size, the liver is larger in the fetus (1/18 of total body weight) than in the adult (1/36 of total body weight) [1].
By ultrasound, a normal liver is less than 16 cm in the midclavicular line [4]. In a study of 2080 patients who underwent transabdominal ultrasonography, the average liver span in the midclavicular line was 14.0 +/- 1.7 cm, with 74 percent having a liver span of 15 cm or less [4]. Fourteen percent had a liver span of 15 to 16 cm, and 12 percent had a liver span of >16 cm. On multivariable analysis, liver span correlated directly with height and body mass index and was greater in men.
Normal anatomy — Classically, the liver is divided into right and left lobes (figure 2). In the normal liver, the right lobe is larger than the left lobe and occupies the right hypochondrium. The smaller left lobe is flatter and is situated in the epigastrium and left hypochondrium.
Blood Supply
The liver receives a dual blood supply; approximately 30 percent of the blood entering the organ is from the hepatic artery, and 70 percent is from the portal vein.
The celiac artery gives rise to the common hepatic artery.The common hepatic artery gives rise to the proper hepatic artery. The proper hepatic artery ascends in the free edge of the lesser omentum. As it approaches the liver it divides near the portal triad into the left and right hepatic arteries. The right hepatic artery gives rise to the cystic artery supplying the gallbladder. The right and left hepatic branches enter the liver and divide into lobar, segmental, and smaller branches.
Eventually blood reaches the arterioles in the portal areas at the periphery of the hepatic lobules and, after providing oxygen and nutrients to the parenchyma, drain into the hepatic sinusoids. The majority of blood entering the liver is venous blood rich in nutrients and molecules absorbed by the gastrointestinal organs. Intrahepatic branches of the portal vein follow the arteries to the portal areas, where portal venules empty into the sinusoids from which molecules are extracted and added. Sinusoidal blood flows to the central vein of each lobule from which increasingly larger veins are formed until typically three hepatic veins exit the liver to join the IVC.

The portal system: 1 = portal vein, 2 = superior mesenteric vein, 3 = splenic vein, 4 = inferior mesenteric vein, 5 = superior rectal vein, 6 = right gastroepiploic vein, 7 = left gastric vein, 8 = esophageal vein, 9 = hepatic veins.
As it approaches the liver, it divides into right and left hepatic branches that enter the liver and divide into lobar, segmental, and smaller branches. Eventually blood reaches the arterioles in the portal areas at the periphery of the hepatic lobules and, after providing oxygen and nutrients to the parenchyma, drain into the hepatic sinusoids. The majority of blood entering the liver is venous blood rich in nutrients and molecules absorbed by the gastrointestinal organs. Intrahepatic branches of the portal vein follow the arteries to the portal areas, where portal venules empty into the sinusoids from which molecules are extracted and added. Sinusoidal blood flows to the central vein of each lobule from which increasingly larger veins are formed until typically three hepatic veins exit the liver to join the IVC (Figure 29-2).
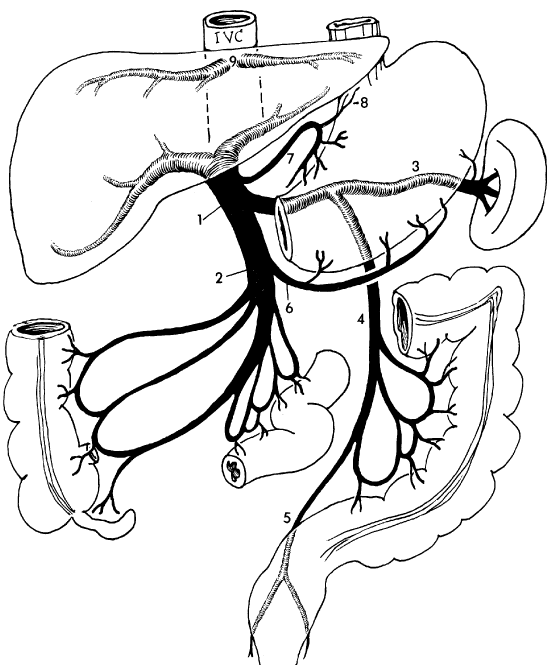
The portal system: 1 = portal vein, 2 = superior mesenteric vein, 3 = splenic vein, 4 = inferior mesenteric vein, 5 = superior rectal vein, 6 = right gastroepiploic vein, 7 = left gastric vein, 8 = esophageal vein, 9 = hepatic veins. (Reproduced, with permission, from the University of Texas Health Science Center Houston Medical School.)
Content 2
Portal Triad
The portal triad lies between the caudate and quadrate lobes and is the structural unit of the liver (Figure 9-2B and C). The portal triad consists of the portal vein, proper hepatic artery, and the common hepatic duct. The portal vein is deep to the hepatic artery and the common hepatic duct.
- Proper hepatic artery. Branches from the celiac trunk via the common hepatic artery. The hepatic artery supplies oxygenated blood to the liver. The cystic artery arises from the hepatic artery to supply the gallbladder.
- Portal vein. Formed through the union of the splenic and superior mesenteric veins, deep to the pancreas. The portal vein collects nutrient-rich venous blood from the small and large intestines, where it is transported to the hepatic sinusoids of the liver for filtration and detoxification. The hepatic sinusoids empty into the common central vein, which empties into the hepatic veins and ultimately drains into the inferior vena cava. The flow of blood from one capillary bed (intestinal capillaries) through a second capillary bed (liver sinusoids) before its return by systemic veins to the heart is defined as the hepatic portal system.
- Common hepatic duct. The union of the left and right hepatic ducts forms the common hepatic duct. The common hepatic duct transmits bile produced in the liver to the gallbladder for storage.
 Portal hypertension results when there is an obstruction to the regular flow of blood through the sinusoids of the liver. There are many possible causes, including cirrhosis of the hepatocytes (liver cells). Signs of portal hypertension include hemorrhoids and gastroesophageal bleeding, which result from the obstruction of the portal venous blood flow through the liver and the increased flow of blood through alternate routes to reach the inferior vena cava (e.g., rectal and esophageal veins). When these alternate paths receive more blood than normal, the veins dilate, distend, and become more prone to hemorrhage. For example, esophageal varices are distended esophageal veins, resulting from portal hypertension, and may precipitate life-threatening bleeding in the esophagus if hot or cold fluids are ingested or violent coughing occurs.
Portal hypertension results when there is an obstruction to the regular flow of blood through the sinusoids of the liver. There are many possible causes, including cirrhosis of the hepatocytes (liver cells). Signs of portal hypertension include hemorrhoids and gastroesophageal bleeding, which result from the obstruction of the portal venous blood flow through the liver and the increased flow of blood through alternate routes to reach the inferior vena cava (e.g., rectal and esophageal veins). When these alternate paths receive more blood than normal, the veins dilate, distend, and become more prone to hemorrhage. For example, esophageal varices are distended esophageal veins, resulting from portal hypertension, and may precipitate life-threatening bleeding in the esophagus if hot or cold fluids are ingested or violent coughing occurs.
Gallbladder
The gallbladder lies on the visceral surface of the liver, to the right of the quadrate lobe, and stores and concentrates bile secreted by the liver (Figure 9-2A–C). Bile is released into the duodenum when the gallbladder is stimulated after eating a fatty meal. Bile enters the cystic duct, which joins the common hepatic duct, becoming the common bile duct. The common bile duct courses within the hepatoduodenal ligament of the lesser omentum, deep to the first part of the duodenum, where it joins the main pancreatic duct. Together, the common bile duct and the main pancreatic duct enter the second part of the duodenum at the hepatopancreatic ampulla (of Vater). The sphincter of Oddi surrounds the ampulla and controls the flow of bile and pancreatic digestive enzyme secretions into the duodenum.
Gallstones may form in the gallbladder and obstruct the flow of bile, resulting in inflammation and enlargement of the gallbladder. These stones may be composed of bilirubin metabolites, cholesterol, or various calcium salts. They frequently obstruct the gallbladder, causing retention of bile and the risk of rupture into the peritoneal cavity, which ultimately results in peritonitis.
The pancreas is a mixed exocrine-endocrine gland that produces both digestive enzymes and hormones. It is an elongated retroperitoneal organ, with a large head near the duodenum and more narrow body and tail regions that extend to the left.

(a) The main regions of the pancreas are shown in relation to the two pancreatic ducts and the duodenum.
(b) Micrographs show a pancreatic islet and several pancreatic acini. X75 and X200. H&E.
It is firmly fixed by fibrous attachments anterior to the suprarenal aorta and the first and second lumbar vertebrae. Thus, the pain of acute or chronic pancreatitis is situated deep in the epigastric region and frequently radiates to the back.The pancreas has a thin capsule of connective tissue, from which septa extend to cover the larger vessels and ducts and to separate the parenchyma into lobules (Figure 16–8). The secretory acini are surrounded by a basal lamina that is supported only by a delicate sheath of reticular fibers with a rich capillary network. Endocrine function of the pancreas involves primarily smaller cells similar to enteroendocrine cells located in variously sized clusters called the pancreatic islets (islets of Langerhans). These are described with the endocrine organs in Chapter 20.

Normally, the pancreas is about 15 cm long. The organ is covered by a thin capsule of connective tissue that sends septa into it, separating it into lobules.
The exocrine pancreas is drained by a major central duct called the duct of Wirsung, which runs the length of the gland. This duct is normally about 3–4 mm in diameter. In most individuals, the pancreatic duct enters the duodenum at the duodenal papilla alongside the common bile duct. The sphincter of Oddi surrounds both ducts. In about one third of individuals, the duct of Wirsung and the common bile duct join to form a common channel before terminating at the ampulla of Vater.
Many individuals also have a separate accessory pancreatic duct, called the duct of Santorini, that runs from the head and body of the gland to enter the duodenum about 2 cm proximal to the duodenal papilla. This structure is the embryologic remnant of the proximal ductal system of the dorsal pancreatic bud and often joins the main pancreatic duct in the body of the gland.
The pancreas is a retroperitoneal organ located at the L2 vertebral level and contains the following structures:
- Head (including the uncinate process) and neck. Both parts are nestled within the concavity of the duodenum. The head and neck receive their blood supply from the superior pancreaticoduodenal arteries (celiac trunk) and the inferior pancreaticoduodenal arteries (superior mesenteric artery). The head is the thickest part of the gland (2–4 cm) and lies in the curved space between the first, second, and third portions of the duodenum. The uncinate process is the portion of the head that extends to the left behind the superior mesenteric vessels. The neck connects the head and body and sits immediately anterior to the superior mesenteric vessels.
- Body and tail. Both parts are located anterior to the left kidney, with the tail touching the spleen. The body and tail receive their blood supply from the splenic artery (celiac trunk) and pancreatic branches from the superior mesenteric artery. The end of the pancreatic tale, where it touches the spleen, is the only portion of the pancreas that is not retroperitoneal. The body is situated transversely in the retroperitoneal space, bordered superiorly by the splenic artery and posteriorly by the splenic vein. The tail of the pancreas is less fixed in the retroperitoneum and extends toward, and often immediately adjacent to, the hilum of the spleen.

A. Pancreas and duct systems. B. Anterior view of the foregut; the stomach and liver are removed.
The pancreas is a gland that consists of both exocrine tissue (a gland that produces and secretes products locally) and endocrine tissue (a gland that produces and secretes hormones into the blood).
- Pancreas as an exocrine organ. The pancreas produces enzymes that chemically digest carbohydrates, proteins, and fats. These enzymes are produced in the pancreatic exocrine glands and are secreted into the main pancreatic duct, which joins the common bile duct within the wall of the duodenum. An accessory pancreatic duct may open separately into the duodenum, proximal to the common bile duct.
- Pancreas as an endocrine organ. Endocrine tissue islands, called pancreatic islets (of Langerhans), are found within the pancreas and produce the hormones insulin and glucagon. These hormones are secreted into the blood stream via the pancreatic vein, where they are transported by the blood to distant cellular targets.
Innervation most likely plays a limited role in the digestive process. Parasympathetic stimulation of the vagus nerve may increase exocrine digestive secretions. Sympathetic input (T5–T9 spinal cord levels via the greater splanchnic nerve) increases the tone of smooth muscle cells on the neck of the secretory units, thus inhibiting the release of digestive enzymes.
The normal spleen is about 12 cm in length and 7 cm in width and is not normally palpable. CT or ultrasound is a superior test.
The spleen is located in the left upper quadrant of the abdomen, between the greater curvature of the stomach, splenic flexure of the colon, apex of the left kidney, and tail of the pancreas. Its superior surface is roofed by the diaphragm.
It is protected by ribs 9, 10, and 11and is suspended in its location by multiple peritoneal reflections, the splenophrenic, gastrosplenic, splenorenal, and splenocolic ligaments. The gastrosplenic ligament carries the short gastric vessels in its superior aspect and the left gastroepiploic in its inferior aspect. The splenorenal ligament houses the splenic artery and vein, as well as the tail of the pancreas. The tail of the pancreas abuts the splenic hilum in 30% of individuals and is within 1 cm of the hilum in 70%.
The spleen is the size of a fist and stores blood, phagocytizes foreign blood particles, and produces mononuclear leukocytes. It also maintains “quality control” over erythrocytes by the removal of senescent and defective red blood cells. The spleen receives its blood supply from the splenic artery (via the celiac trunk) and venous drainage through the portal vein.
An increase in the number of red blood cells may result in an enlarged spleen (splenomegaly). Splenomegaly can occur in patients who are diagnosed with diseases that change the shape of red blood cells (e.g., malaria); as a result, in these patients, the spleen filters an abnormally high number of red blood cells, which results in enlargement of the spleen.
Although protected by the ribs, the spleen is frequently injured in trauma. In many cases, the force applied to the ribcage pushes the ribs inward, fracturing the ribs, and the free edges puncture the spleen.

The splenic artery, a branch of the celiac trunk, is a tortuous vessel that gives off multiple branches to the pancreas as it travels along its posterior aspect. There are two typical arrays of the splenic artery—the magistral, which branches into terminal and polar arteries near the hilum of the spleen and the distributed, which, as the name implies, gives off its branches early and distant from the hilum. There is typically a superior polar artery, which sometimes communicates with the short gastric arteries, superior, middle, and inferior terminal arteries, and an inferior polar artery. Knowing these variable distributions is necessary when performing resections, especially a spleen-preserving procedure. Because of the variable nature of the splenic artery, one must be cautious when operating near this vessel and its tributaries.
The spleen is encased within a fibroelastic capsule. Trabeculae that compartmentalize the spleen pass from the splenic capsule. The spleen is also segmented by the divisions of the splenic vessels as they branch within the organ and merge with these trabeculae. The arterioles branch into even smaller vessels and leave these trabeculae to merge with the splenic pulp, where their adventitia is replaced by a covering of lymphatic tissue that continues until the vessels thin to capillaries. These lymphatic sheaths make up the white pulp of the spleen and are interspersed among the arteriolar branches as lymphatic follicles. The white pulp then interfaces with the red pulp at the marginal zone. It is in this marginal zone that the arterioles lose their lymphatic tissue and the vessels evolve into thin-walled splenic sinuses and sinusoids. The sinusoids then merge into venules, draining into veins that travel along the trabeculae to form splenic veins that mirror their arterial counterparts. The splenic vein leaves the splenic hilum, travels posteriorly to the pancreas, joining with pancreatic branches and often the inferior mesenteric vein to finally receive the superior mesenteric vein forming the portal vein.
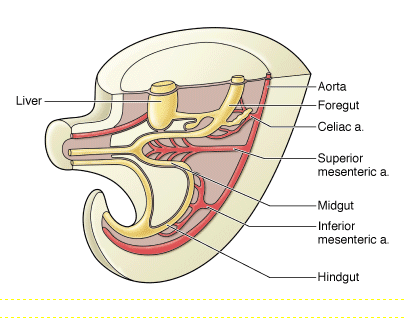
There are three unpaired arterial trunks that arise from the anterior surface of the abdominal aorta respectively for the foregut, midgut and the hindgut. Each receives a primary, but not sole, arterial supply: foregut–celiac trunk, midgut–superior mesenteric artery, and hindgut–inferior mesenteric artery.
The foregut organs are the stomach, the first half of the duodenum, and the liver, gallbladder, pancreas, and spleen.
Arterial Supply
The principal blood supply to the organs of the foregut is the celiac trunk. The celiac trunk is an unpaired artery arising from the abdominal aorta, immediately below the aortic hiatus of the diaphragm at the T12 vertebral level. The celiac trunk divides into the left gastric, splenic, and common hepatic arteries ( See Figure A).
- Left gastric artery. The smallest branch of the celiac trunk. The left gastric artery provides blood supply to the lesser curvature of the stomach and the inferior portion of the esophagus.
- Splenic artery. The largest branch of the celiac trunk. The splenic artery provides blood to the spleen, the greater curvature of the stomach (left gastroomental branch), the fundus (short gastric branches), and the pancreas (pancreatic branches). The splenic artery follows a highly tortuous course along the superior border of the pancreas.
- Common hepatic artery. Divides into the proper hepatic artery, the gastroduodenal artery, and the right gastric artery.
- Proper hepatic artery. Ascends in the free edge of the lesser omentum and divides near the portal triad into the left and right hepatic arteries. The right hepatic artery gives rise to the cystic artery, supplying the gallbladder.
- Right gastric artery. Supplies the lesser curvature of the stomach and usually forms an anastomosis with the left gastric artery.
- Gastroduodenal artery. Descends deep to the first part of the duodenum, giving rise to the following two principal branches:
- Right gastroomental artery. Supplies the right half of the greater curvature of the stomach.
- Superior pancreaticoduodenal artery. Courses between the duodenum and the head of the pancreas to further split into anterior and posterior divisions.

Venous Drainage
The principal venous drainage of the foregut is to the portal venous system (Figure B). The portal venous system drains nutrient-rich venous blood from the gastrointestinal tract and the spleen to the liver. Three collecting veins converge to form the portal vein: the splenic vein and the superior mesenteric and inferior mesenteric veins. Portal venous blood flows to the liver, where nutrients are metabolized. The metabolic products are collected in central veins, which are tributaries of the hepatic veins. The hepatic veins emerge from the liver to drain into the inferior vena cava. The portal and hepatic veins are connected within the liver, at the liver lobules; thus, the combined venous system is called the hepatic portal system of veins.
The blood passes through sinusoids lined by single-layered sheets of hepatocytes. The sinusoids are fenestrated, allowing easy access of the products of digestion into hepatocytes. The sinusoids drain into central veins, which empty into the hepatic veins and finally to the IVC. Note that blood drains away from the portal triad toward the central vein, whereas bile flows in the opposite direction toward the portal triad and bile ducts.
Content 7
Abdominal Venous Drainage
Blood in the abdomen drains back to the heart via two routes: caval drainage and portal drainage (Figure C).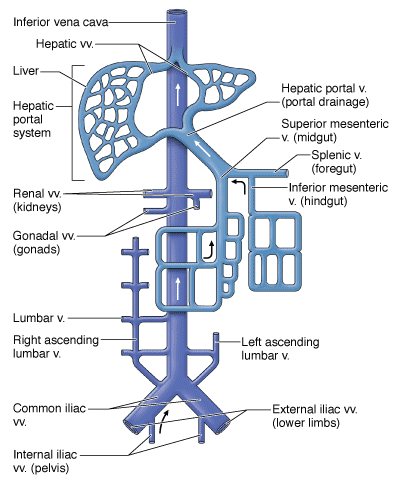
Caval Drainage
Venous blood that is returned to the heart from the anterior and posterior abdominal walls and the retroperitoneal organs via the superior or inferior vena cava.
- Inferior epigastric veins. Return blood to the heart via the inferior vena cava.
- Intercostal veins. Return blood to the heart via the superior vena cava.
- Lumbar veins. Return blood to the heart directly via the inferior vena cava or indirectly via the superior vena cava (lumbar veins may drain into the ascending lumbar veins to the azygos system of veins to the superior vena cava).
Portal Drainage
Venous blood from the gut tube and its derivatives returns to the heart via the hepatic portal vein to the liver. In other words, venous blood from the gut tube reaches the inferior vena cava after coursing through the liver.
- Foregut. Branches from the gastric and splenic veins to the portal vein.
- Midgut. Branches from the superior mesenteric vein to the portal vein.
- Hindgut. Branches from the inferior mesenteric vein to the portal vein.
Abdominal Lymphatics
Lymphatics generally follow neurovascular bundles throughout the body. Clusters of lymph nodes, which are important in monitoring the immune system, are found along the course of the lymphatics. The central lymph nodes in the abdomen are named according to their associated artery. For example, the lymph nodes clustered at the origin of the celiac trunk are called celiac lymph nodes.
Innervation of the Gut Tube
The regions of the gut tube receive the following autonomic innervation:
- Foregut. Sympathetics from the greater splanchnic nerves (T5–T9). Parasympathetics from the vagus nerves.
- Midgut. Sympathetics from the lesser splanchnic nerves (T10–T11). Parasympathetics from the vagus nerves.
- Hindgut. Sympathetics from the lumbar splanchnic nerves. Parasympathetics from the pelvic splanchnics (S2–S4 spinal cord levels).
The portal system drains venous blood from the distal end of the esophagus, stomach, small and large intestines, proximal portion of the rectum, pancreas, and spleen or metabolic processing before the blood returns to the heart. It is relevant for first-pass metabolism of medications and explains why GI cancers tend to metastasize to the liver. It is so vascular that it is the most common organ to have metastases from other malignancies. A malignancy found in the liver is more likely to be of metastatic than primarily hepatic origin, especially if there are multiple growths.
The portal system is the venous counterpart to areas supplied by the celiac trunk and the superior and inferior mesenteric arteries.
Blood Flow of the Portal System
The liver is unique in that it receives both nutrient-rich deoxygenated blood (portal vein) and oxygenated blood (hepatic arteries). The portal vein branches as it enters the liver, where its blood percolates around hepatocytes in tiny vascular channels known as sinusoids. Hepatocytes detoxify the blood, metabolize fats, carbohydrates, and drugs, and produce bile. The sinusoids receive deoxygenated blood from the portal veins (provide blood for metabolism and detoxification) and oxygenated blood from the hepatic arteries (provide oxygen for hepatocytes). Blood exits the sinusoids into a central vein, which empties into the hepatic veins and ultimately into the inferior vena cava, which passes through the diaphragm before entering the right atrium of the heart.
Oral drugs travel throughout the gastrointestinal tract, where they are absorbed by the small intestine. These drugs then travel to the liver via the hepatic portal system, where they are metabolized before entering the systemic circulation. Because of hepatic metabolism, the concentration of oral drugs is reduced before entering the systemic circulation. This is known as the first-pass effect. Therefore, drugs that are inactivated by the liver (e.g., nitroglycerin) must be administered by a different method. For example, nitroglycerin is administered sublingually (absorption under the tongue) because, if swallowed, the liver inactivates the drug before it can enter the systemic circulation.
Veins of the Portal System
Veins of the portal system generally mirror the arterial branches of the celiac trunk and the superior and inferior mesenteric arteries. The major veins of the portal system are as follows:
- Splenic vein. Drains blood from the foregut, including the spleen, pancreas, and part of the stomach. The splenic vein courses deep to the pancreas.
- Superior mesenteric vein. Drains blood from the midgut and part of the foregut. The superior mesenteric vein is located to the right of the superior mesenteric artery as it courses over the third part of the duodenum.
- Gastro-omental veins. Drain blood from the greater curvature of the stomach into the superior mesenteric vein.
- Inferior mesenteric vein. Drains blood from the hindgut, including the proximal third of the rectum. The inferior mesenteric vein usually drains into the superior mesenteric vein, inferior to its union with the portal vein.
- Portal vein. Collects blood from the foregut, midgut, and hindgut. The portal vein is located deep to the hepatic artery and cystic duct and is formed by the union of the superior mesenteric vein and splenic vein, deep to the neck of the pancreas.
- Gastric veins. Drain blood from the lesser curvature of the stomach into the portal vein.

A. The portal venous system. B. The three primary portal–caval anastomoses.
Portal–Caval Anastomoses
To better understand the portal–caval anastomoses, recall that veins in the abdomen return blood to the heart via two routes:
- Portal system. Veins from the foregut, midgut, and hindgut drain blood to the liver before the blood enters the inferior vena cava and ultimately returns to the heart.
- Caval system. Veins from the lower limbs, pelvis, and posterior abdominal wall transport blood directly to the inferior vena cava before the blood returns to the heart.
Portal–caval anastomoses occur at regions of the gastrointestinal tract that are drained by both the portal and systemic (-caval) systems. The principal portal–caval anastomoses are as follows:
-
Distal portion of the esophagus. The left gastric vein of the hepatic portal system drains blood from the distal portion of the esophagus. However, most of the blood drained from the esophagus is through the esophageal veins, which drain into the azygos (caval) vein.
-
Anterior abdominal wall. The paraumbilical veins drain the tissue surrounding the umbilicus: Embryologically, these veins communicated with the umbilical veins. These connections may reopen during chronic portal hypertension. Normally in the adult, most of the venous drainage is from the inferior epigastric veins.
-
Rectum. The proximal portion of the rectum is drained via the superior rectal vein, which drains into the inferior mesenteric vein of the hepatic portal system. However, the remainder of the rectum is drained by the middle rectal vein (branch of the internal iliac vein) and inferior rectal vein (branch of the internal pudendal vein).
When hepatocytes are damaged (e.g., due to disease, alcohol, or drugs), the liver cells are replaced by fibrous tissue, which impedes the flow of blood through the liver (cirrhosis). When the hepatic portal system is blocked, the return of blood from the intestines and spleen through the liver is impeded, resulting in portal hypertension. Therefore, veins that usually flow into the liver are blocked. Consequently, blood pressure in the blocked veins increases, causing them to dilate and gradually reopen previously closed connections with the caval system. Veins in the distal portion of the esophagus begin to enlarge (esophageal varices); veins in the rectum begin to enlarge (internal hemorrhoids); and in chronic cases, the veins of the paraumbilical region enlarge (caput medusa).